


Introduction
Choosing brackets for children requires more than picking a standard appliance. In pediatric dentistry, smaller teeth, mixed dentition, comfort concerns, and variable cooperation all affect how well a bracket system performs over time. The right option can improve control of tooth movement, reduce irritation to soft tissues, and make hygiene and follow-up visits more manageable for both clinician and patient. This article outlines the key features that matter most when comparing orthodontic brackets for younger patients, including size, profile, bonding reliability, and treatment efficiency, so readers can better understand which designs are best suited to pediatric care.
Why Orthodontic Brackets Matter in Pediatric Dentistry
Orthodontic brackets serve as the foundational mechanical interface in pediatric orthodontic treatments. Applying fixed appliances to children and adolescents presents unique challenges, including smaller clinical crowns, mixed dentition, and varying levels of patient compliance. Selecting the appropriate bracket system is not merely a matter of clinical preference; it dictates the biomechanical control of tooth movement and the overall patient experience throughout the treatment lifecycle.
Impact on treatment efficiency and comfort
The design and profile of orthodontic brackets directly influence the efficiency of tooth movement and the physical comfort of the pediatric patient. Advanced bracket designs, such as those with highly polished surfaces and rounded contours, minimize friction between the archwire and the bracket slot. This reduction in sliding resistance can decrease overall chair time by 15% to 20% during routine adjustments. Furthermore, smoother profiles mitigate the risk of soft tissue ulcerations, which is critical for maintaining compliance and oral hygiene in younger patients.
Clinical factors in bracket selection
Clinical selection relies heavily on anatomical compatibility and the bracket’s retentive features. Pediatric patients often present with partially erupted permanent teeth or primary teeth that require temporary bonding. Brackets featuring an 80-gauge foil mesh base provide an optimal surface area for adhesive penetration, ensuring secure attachment even on compromised enamel surfaces. Additionally, built-in prescriptions—such as specific torque and angulation values—must align with the developmental stage of the patient’s dentition to prevent unintended root resorption.
Commercial factors in bracket selection
Beyond clinical efficacy, commercial factors play a pivotal role in the procurement of orthodontic brackets for high-volume pediatric practices. Inventory management requires balancing the cost per unit against clinical reliability. Manufacturers typically impose a Minimum Order Quantity (MOQ) ranging from 50 to 100 sets for bulk pricing tiers. Practices must evaluate the shelf life of pre-pasted brackets and the logistical footprint of maintaining multiple prescription types, ensuring that capital is not tied up in rarely used inventory.
Types of Orthodontic Brackets for Pediatric Patients

The orthodontic industry offers a diverse array of bracket systems, each engineered to address specific biomechanical and aesthetic requirements. For pediatric patients, the choice of material and ligation method must balance durability with the unique constraints of developing dentition.
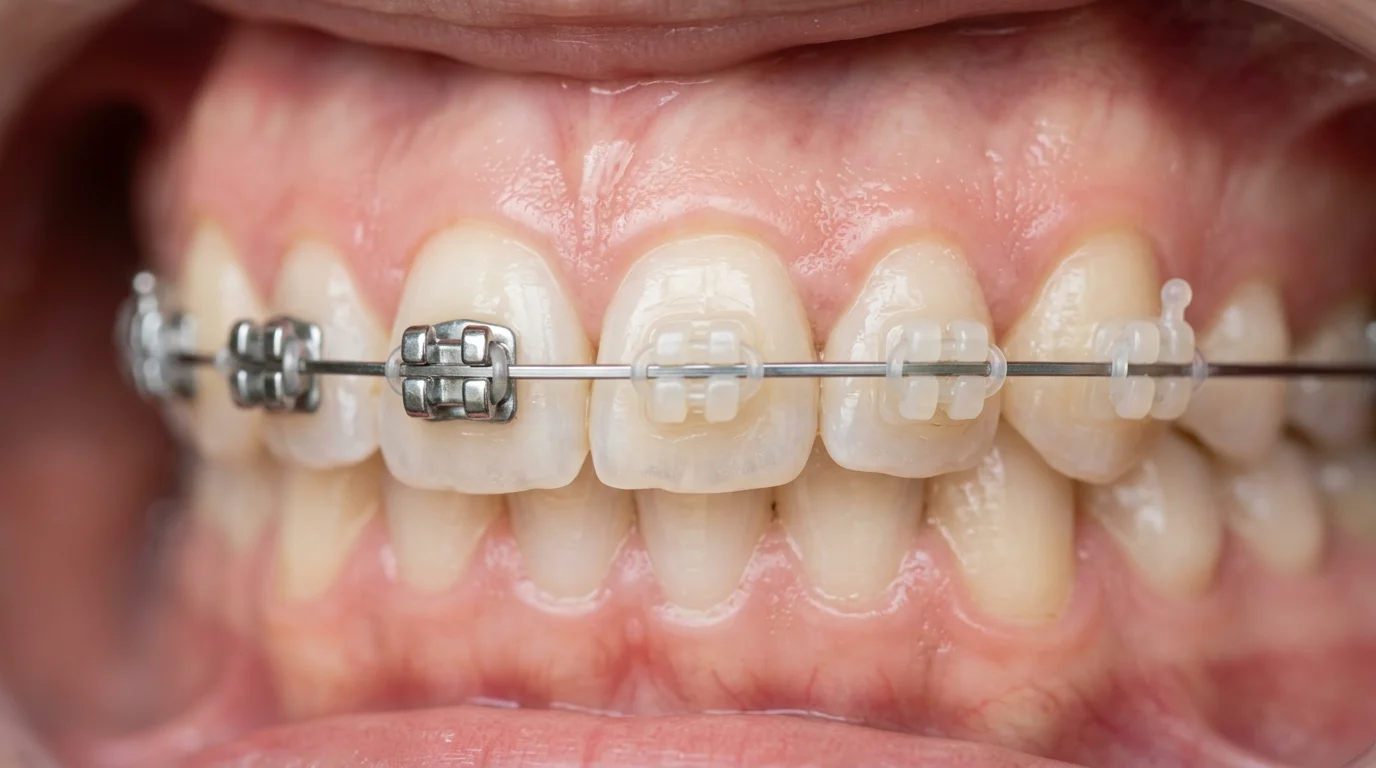
Metal, ceramic, self-ligating, and low-profile options
Traditional stainless steel brackets remain the industry standard due to their high yield strength and resistance to deformation under masticatory forces. Ceramic brackets offer an aesthetic alternative, utilizing polycrystalline or monocrystalline alumina to blend with the natural tooth color, though they carry a higher risk of fracture. Self-ligating brackets—available in both active and passive designs—eliminate the need for elastomeric ties, reducing friction and plaque accumulation. Low-profile variations of these materials are particularly beneficial for children, as they project less prominently from the tooth surface, reducing mucosal irritation.
Key features for mixed dentition and limited enamel
Mixed dentition phases require brackets that can accommodate transitional anatomy and limited enamel surface areas. Pediatric crowns are shorter, necessitating brackets with a reduced occlusogingival dimension to avoid occlusal interference. An optimal bracket base surface area for pediatric molars and premolars typically falls between 9 and 11 square millimeters. This specific sizing ensures adequate bond strength without encroaching on the gingival margin, which is vital for preventing hypertrophic gingival tissue responses commonly seen in adolescents.
Durability, comfort, and cost comparison
Evaluating the trade-offs between different bracket types involves analyzing durability, patient comfort, and procurement costs. Stainless steel systems are highly durable and cost-effective, whereas ceramic and self-ligating systems command a premium due to complex manufacturing processes.
| Bracket Type | Durability / Fracture Resistance | Friction Level | Estimated Cost per Set (USD) |
|---|---|---|---|
| Standard Metal | Very High | Moderate (with elastomers) | $15.00 – $25.00 |
| Ceramic (Aesthetic) | Moderate (Brittle) | High | $35.00 – $55.00 |
| Self-Ligating (Metal) | High | Very Low | $45.00 – $70.00 |
| Low-Profile Metal | High | Moderate | $20.00 – $30.00 |
Cost variations depend on the region of manufacture and the specific metallurgical composition of the bracket.
How to Evaluate Orthodontic Brackets for Pediatric Use
Rigorous evaluation of orthodontic brackets is essential to ensure they meet both clinical demands and international safety regulations. For pediatric applications, the focus must center on material safety, precision engineering, and predictable mechanical behavior during both bonding and debonding phases.
Materials, biocompatibility, and manufacturing standards
Orthodontic brackets are primarily manufactured from 17-4 PH (precipitation-hardening) stainless steel, known for its optimal balance of strength and corrosion resistance. However, traditional stainless steel alloys contain 8% to 10% nickel, which can trigger allergic contact stomatitis in sensitized pediatric patients. In such cases, titanium or specialized nickel-free alloys are mandatory. Compliance with global medical device manufacturing protocols, such as ISO standards, ensures that materials undergo strict biocompatibility testing, mitigating the risk of heavy metal leaching into the oral environment.
Bond strength, debonding behavior, and slot precision
The mechanical interface between the bracket, adhesive, and enamel dictates the success of the appliance. Shear bond strength (SBS) is a critical metric; the optimal SBS for orthodontic brackets ranges from 6 to 8 Megapascals (MPa). Values below 6 MPa result in frequent bond failures, disrupting treatment, while values exceeding 8 MPa increase the risk of enamel tear during the debonding process. Furthermore, slot precision is paramount for accurate torque expression. High-quality brackets maintain slot dimension tolerances of +/- 0.001 inches, ensuring that the archwire engages exactly as prescribed by the orthodontist.
How to Choose the Right Orthodontic Brackets
Establishing a standardized procurement protocol for orthodontic brackets ensures clinical consistency and stabilizes supply chain costs. Dental practices and institutional buyers must implement a systematic approach to select, evaluate, and source these critical medical devices.
Step-by-step bracket selection criteria
The first step in bracket selection involves defining the clinical baseline: identifying the preferred prescription (such as Roth or MBT) and the specific slot size (typically 0.018-inch or 0.022-inch). Next, practices must analyze their patient demographic to determine the necessary ratio of standard metal to aesthetic or self-ligating brackets. Buyers should establish a target budget, factoring in not just the initial purchase price, but the hidden costs of bracket failures and extended chair time. Ordering small sample batches for clinical trial periods allows practitioners to verify handling characteristics before committing to high-volume contracts.
How to compare suppliers and product consistency
Supplier evaluation requires scrutinizing both product consistency and logistical reliability. Quality control can be assessed by tracking the defect rate of incoming shipments; a reliable manufacturer should maintain a defect rate of less than 1% (e.g., deformed slots, detached mesh bases). Supply chain resilience is equally important. Institutional buyers should look for suppliers offering consistent lead times of 2 to 4 weeks to prevent inventory shortages. Monitoring international trade metrics can also help buyers anticipate regional supply disruptions or tariffs that might impact the landed cost of imported bracket systems.
Recommendation framework for final decisions
To finalize procurement decisions, dental organizations should utilize a structured recommendation framework that weighs clinical performance against supplier metrics.
| Evaluation Criterion | Key Metric / Threshold | Strategic Importance |
|---|---|---|
| Clinical Precision | Slot tolerance within +/- 0.001 inches | Ensures predictable tooth movement and reduces wire-bending adjustments. |
| Material Safety | Nickel-free options available; ISO certified | Protects pediatric patients from allergic reactions and ensures regulatory compliance. |
| Mechanical Retention | Optimal Shear Bond Strength (6-8 MPa) | Minimizes emergency visits for broken brackets while safeguarding enamel upon removal. |
| Supplier Reliability | Lead time < 4 weeks; Defect rate < 1% | Stabilizes inventory management and prevents costly clinical delays. |
By applying this framework, practices can secure orthodontic brackets that deliver consistent clinical outcomes while maintaining financial and operational efficiency.
Key Takeaways
- The most important conclusions and rationale for Orthodontic Brackets
- Specs, compliance, and risk checks worth validating before you commit
- Practical next steps and caveats readers can apply immediately
Frequently Asked Questions
Which bracket type is usually best for children?
Low-profile metal brackets are often the most practical choice. They are durable, cost-effective, and less likely to irritate cheeks and lips in younger patients.
Are self-ligating brackets better for pediatric patients?
They can be helpful when lower friction and easier cleaning are priorities. Self-ligating designs also reduce elastomer use, which may lower plaque buildup around brackets.
When should ceramic brackets be considered for kids?
Choose ceramic brackets when appearance matters and the child can follow care instructions well. They blend with teeth but are more brittle and usually cost more than metal options.
What bracket features matter most in mixed dentition cases?
Look for a smaller occlusogingival size, reliable mesh base bonding, and prescriptions suited to developing teeth. These features help fit short crowns and improve bond strength on limited enamel.
Where can clinics source pediatric orthodontic brackets in bulk?
Practices can review bracket options on DenRotary, including metal, ceramic, and self-ligating systems. Check MOQ, prescription availability, and inventory needs before placing a bulk order.

Post time: May-27-2026