



Introduction
In complex tooth alignment, wire selection is not a minor material choice; it shapes force delivery, treatment efficiency, and patient comfort from the first appointment onward. Severe crowding, deep bites, and displaced teeth place very different demands on an orthodontic wire than routine cases, especially when controlled, continuous force is needed over a wide range of activation. This article explains how dental arch wire properties affect biomechanics in difficult cases, which wire types are best suited to different treatment phases, and what clinical trade-offs matter most when balancing flexibility, springback, control, and long-term results.
Why wire choice matters in orthodontic treatment
The selection of an orthodontic wire serves as the primary engine for tooth movement, dictating the biomechanical forces applied to the periodontal ligament. In complex alignment cases, where severe crowding, deep bites, or high-angle discrepancies are present, the arch wire must deliver highly controlled, continuous forces to achieve predictable outcomes.
Choosing the wrong wire can compromise the entire treatment plan, leading to inefficient mechanics, patient discomfort, and extended treatment timelines. Understanding the precise biomechanical requirements of each treatment phase is essential for clinical success.
How complex tooth alignment changes wire requirements
Severe malocclusions alter the fundamental requirements for arch wires. In cases with significant vertical or horizontal discrepancies, the wire must exhibit exceptional flexibility and high springback to engage severely displaced teeth without undergoing permanent plastic deformation.
Biologically, the optimal force for initiating tooth movement without causing tissue necrosis ranges between 50 and 150 grams. Complex alignments demand wires capable of maintaining this light, continuous force across a wide deflection range. When engaging a tooth displaced by more than 3 millimeters, conventional stainless steel would exert excessive force, whereas superelastic alloys can maintain the required 50-150 gram threshold even at maximum deflection.
What clinical and commercial risks come from poor wire selection
Selecting an inappropriate wire introduces significant clinical and commercial liabilities. Clinically, applying forces exceeding 200 grams through an overly stiff wire increases the risk of root resorption, periodontal ischemia, and loss of anchorage. Such complications not only harm the patient but also severely disrupt the treatment sequence.
Commercially, poor wire selection directly impacts a practice’s profitability. Wire breakages or the need for unscheduled adjustments due to lost ligations can increase chair time by 15 to 20 minutes per unexpected visit. Furthermore, inefficient biomechanics can extend total treatment time by 3 to 6 months, reducing the overall case profitability and limiting the clinic’s capacity to accept new patients.
How to evaluate orthodontic wire options
Evaluating the array of available arch wires requires a systematic analysis of their metallurgical properties and clinical behavior. Practitioners must balance flexibility, stiffness, and formability to match the specific physiological demands of the patient’s dentition.
Modern orthodontics relies on three primary alloy families, each engineered to perform specific biomechanical tasks during different phases of the treatment cycle.
How wire materials compare
The three dominant materials in orthodontic wires possess distinct mechanical profiles that dictate their clinical application. Nickel-Titanium (NiTi) is favored for its superelasticity, Stainless Steel (SS) for its rigidity, and Beta-Titanium (TMA) for offering an intermediate balance.
| Material | Modulus of Elasticity (GPa) | Yield Strength (MPa) | Primary Clinical Phase |
|---|---|---|---|
| Nickel-Titanium (NiTi) | ~35 | ~300 – 600 | Initial leveling and aligning |
| Beta-Titanium (TMA) | ~65 | ~1,000 | Intermediate mechanics, detailing |
| Stainless Steel (SS) | ~160 | ~1,500 | Space closure, finishing, torque |
This substantial difference in the modulus of elasticity means that a stainless steel wire will deliver roughly four to five times the force of a NiTi wire of the exact same cross-sectional dimensions. Understanding this differential is critical when transitioning between materials.
Which wire properties matter most in difficult cases
In difficult cases, the load-deflection rate and frictional resistance are the most critical properties. A low load-deflection rate ensures that the force delivered to the tooth remains relatively constant regardless of how far the wire is bent to engage the bracket.
Thermal properties also play a vital role, particularly with Copper NiTi (CuNiTi) variants. By adjusting the alloy composition, manufacturers can set the austenitic transformation temperature. Wires calibrated to activate at 27°C, 35°C, or 40°C allow practitioners to tailor the force levels to the patient’s oral environment, providing lighter forces for periodontally compromised patients when using a 40°C wire.
What criteria help compare wire options
Beyond mechanical properties, clinical evaluation must incorporate practical procurement criteria. The cost per arch wire can vary dramatically, ranging from $1.50 for standard stainless steel to over $12.00 for specialized thermal-activated or aesthetically coated wires.
Practices must also evaluate the reliability and quality control of the orthodontic wire supplier. Key criteria include the consistency of the arch form across different batches, the resilience of aesthetic coatings against salivary degradation, and the guaranteed shelf life of thermal-activated alloys, which can degrade if stored improperly over several years.
How to match arch wire selection to treatment needs
Arch wire selection is not a static decision; it is a dynamic progression that mirrors the phases of orthodontic treatment. Properly matching the wire to the immediate clinical objective minimizes friction, maximizes control, and ensures a smooth transition toward the final occlusion.
Which dimensions, cross-sections, and arch forms to choose
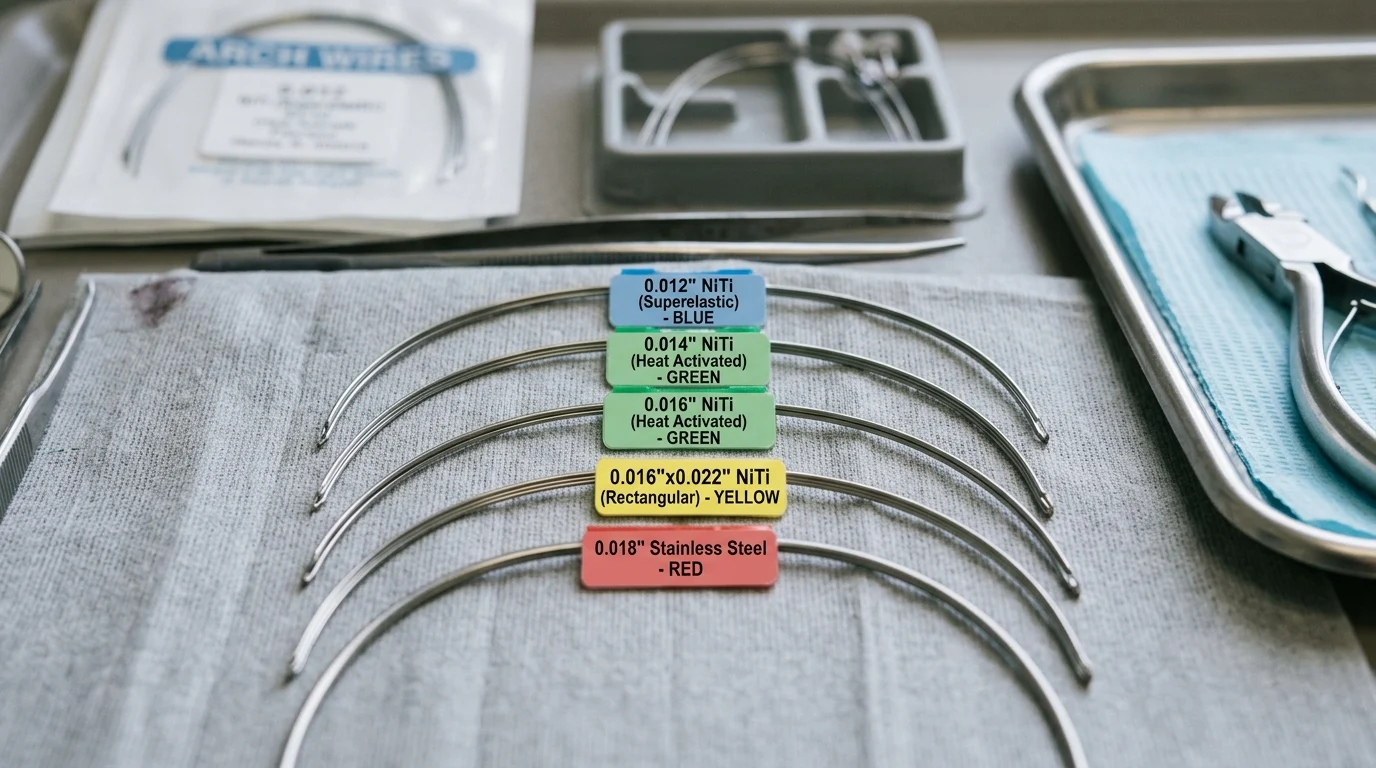
Wire dimensions directly control the amount of play or clearance within the bracket slot. Round wires, typically ranging from 0.012 inches to 0.018 inches in diameter, are utilized primarily for unbinding crowded teeth and initiating leveling. Rectangular wires, ranging from 0.016 x 0.022 inches to 0.019 x 0.025 inches, are essential for three-dimensional control, specifically torquing the roots.
Arch forms must also be carefully selected to respect the patient’s original biological boundaries. Utilizing a broad square arch form on a naturally tapered mandible can lead to unstable expansion and subsequent relapse. Maintaining intercanine width within 1 to 2 millimeters of the original dimension is a standard threshold for long-term stability.
What wire sequence supports efficient treatment progression
An efficient wire sequence minimizes the number of wire changes while maximizing the biological response. A typical progression for a 0.022-inch slot system involves distinct phases designed to seamlessly transfer control from flexible to rigid alloys.
| Treatment Phase | Wire Dimension & Material | Average Duration | Clinical Goal |
|---|---|---|---|
| Initial Leveling | 0.014″ or 0.016″ Superelastic NiTi | 8 – 12 weeks | Resolve severe crowding, correct rotations |
| Intermediate | 0.016″ x 0.022″ Thermal NiTi | 6 – 10 weeks | Initiate torque, complete leveling |
| Working/Space Closure | 0.019″ x 0.025″ Stainless Steel | 12 – 24 weeks | Maintain arch form, close extraction spaces |
| Finishing | 0.017″ x 0.025″ TMA | 4 – 8 weeks | Final detailing, root parallelism |
This structured sequence ensures that forces are gradually increased, allowing the periodontal tissues adequate time to remodel and preventing the hyalinization that slows down tooth movement.
When to adjust wire selection during treatment
Clinical adjustments to the planned wire sequence are frequently necessary. If a practitioner observes excessive friction or binding that halts sliding mechanics, stepping down to a smaller dimension or switching to a lower-friction material is required.
Conversely, if torque expression is inadequate, the wire must fill more of the bracket slot. For effective torque expression in a 0.022-inch slot, a wire dimension of at least 0.019 x 0.025 inches is typically required, leaving a functional clearance of roughly 0.002 to 0.003 inches, which translates to about 7 to 10 degrees of torque play.
What quality and compliance factors affect wire selection
The biomechanical performance of an arch wire is heavily dependent on microscopic manufacturing tolerances and strict adherence to international quality standards. Variations in surface topography or dimensional accuracy can drastically alter clinical outcomes.
How to assess manufacturing consistency and surface finish
Manufacturing consistency is best evaluated through dimensional tolerance and surface finish. High-quality wires maintain strict dimensional tolerances, typically within ±0.0005 inches. A deviation larger than this can result in unexpected loss of torque control or excessive binding within the bracket slot.
Surface finish directly impacts the coefficient of friction. Wires subjected to advanced electropolishing exhibit surface roughness (Ra) values below 0.15 micrometers. Compared to untreated wires with Ra values above 0.30 micrometers, these highly polished surfaces can reduce sliding friction by up to 30%, significantly accelerating space closure mechanics.
Which regulatory and material standards matter
Compliance with international standards guarantees both mechanical reliability and patient safety. The primary benchmark is ISO 15841, which specifies the dimensional and mechanical testing requirements for orthodontic wires, ensuring predictable springback and yield strength across batches.
Biocompatibility is governed by ISO 10993. Given that NiTi alloys contain roughly 50% nickel, evaluating the material’s resistance to corrosion is critical. Compliant wires possess a stable titanium oxide passivation layer that limits nickel ion leaching to well below the safety threshold of 0.2 µg/cm² per week, mitigating the risk of allergic reactions in sensitive patients.
How to make the final wire selection decision
Finalizing the arch wire sequence requires a strategic balance between individualized patient care and the logistical realities of running a dental practice. A streamlined approach prevents inventory bloat while ensuring the clinician has the exact tools needed for complex mechanics.
What decision framework balances treatment goals and inventory needs
An effective decision framework standardizes the core wire sequence while allowing modular additions for complex cases. By standardizing 80% of treatments to a core set of 4 to 5 wire SKUs (Stock Keeping Units), clinics can reduce inventory holding costs by 15% to 20% and minimize the risk of expired thermal wires.
When a complex case presents, the clinician can then selectively order specialized items, such as multi-force NiTi or specific aesthetic wires. Partnering with a reliable dental arch wire supplier ensures that these specialty wires can be procured quickly without needing to maintain large, slow-moving stockpiles.
Which selection mistakes practices should avoid
Practices must actively avoid common selection errors that compromise treatment. One frequent mistake is skipping intermediate wire sizes to rush treatment. Jumping directly from a 0.014-inch NiTi to a 0.018 x 0.025-inch Stainless Steel wire can generate forces exceeding 300 grams, risking severe root resorption and bracket debonding.
Another critical error is prioritizing unit cost over material compliance. Purchasing non-compliant or counterfeit wires often results in higher defect rates, such as premature intraoral fracturing or rapid loss of superelastic properties. The nominal savings of $1 per wire are quickly erased by the cost of additional chair time and delayed treatment objectives.
Further reading:
Key Takeaways
- The most important conclusions and rationale for orthodontic wire,dental arch wire
- Specs, compliance, and risk checks worth validating before you commit
- Practical next steps and caveats readers can apply immediately
Frequently Asked Questions
Which orthodontic wire is best for severe crowding at the start of treatment?
Superelastic NiTi is usually best for initial alignment because it engages displaced teeth easily and delivers light, continuous force over wide deflections.
When should a clinician switch from NiTi to stainless steel arch wire?
Switch when initial leveling is complete and more rigid control is needed for space closure, finishing, or torque expression.
Why is beta-titanium wire useful in complex tooth alignment cases?
Beta-titanium offers a middle ground between NiTi and stainless steel, giving good formability with moderate stiffness for detailing and controlled mechanics.
How do thermal-activated CuNiTi wires help sensitive or compromised cases?
They activate at set temperatures and can provide gentler force levels, which is helpful for periodontally compromised or more discomfort-prone patients.
What should buyers check when sourcing orthodontic wire from suppliers like DenRotary?
Check alloy consistency, size tolerance, force performance, packaging quality, and reliable product availability to reduce breakage, chairside delays, and replacement issues.

Post time: Jun-15-2026